Presenting dental treatment plans to patients seems like this daunting, nerve wrecking process because you think you have to “sell” the patient on the treatment.
Well I’m here to change that perception.
This video is for you if you’re the doctor, the manager, the treatment coordinator or anyone involved in the dental front office administration – who is responsible for presenting treatment plans to patients.
I’ll be splitting this topic of Presenting treatment plans and Financial presentation into two parts.
For this video, I’ll focus on explaining the Treatment plan to the patients, and for the next video, I’ll focus on presenting the finances.
I’m not going to focus on the clinical aspect of the treatment plan meaning – what should be recommended to a patient based on diagnosis from exam and xrays.
I’m going to assume you’ve done the diagnosis, and have a treatment plan in place and now it’s time to present it to the patient.
Let’s get started!
When to present Treatment Plans
For the Doctor
If you’re the doctor presenting treatment plans to patients like I do in my own practice (because I don’t have a treatment coordinator) – a treatment plan is to be presented to patients AFTER you’ve gone over the clinical findings with the patient.
Once a diagnosis of their oral health condition has been formed, presenting a dental treatment plan happens after you or your assistant have entered the needed treatment into the Practice Management software (PMS) along with sequence of the treatment.
For Treatment Coordinators and Other Front office personnel
Presenting treatment plans happens either in the operatory once the doctor and/or the hygienist has left the room, or maybe you have a separate consultation room where you present treatment.
Wherever it is, by the time you’re ready to present treatment, you’re going to assume there are procedure codes and treatment sequence already entered into the PMS.
Make sure any intra-oral photographs taken during the clinical exam are transferred to the PMS, so you have easy access should you feel the need to bring them up during your presentation to the patient.
For team members who are new to the dental world, it’s important that you understand the clinical terminology used on a daily basis.
It will make your job easier to explain things in layman’s terms your patients understand. If you don’t understand it, don’t expect your patients to understand it either.
So make sure you ask your clinical team prior to presenting treatment if there’s any confusion.
Staying Organized
When the patient is in front of you ready to have the treatment plan explained to them, there should be NO distractions.
Everything needs to be easily accessible from the computer:
- Treatment plan with procedures and sequence of treatment
- intra-oral photographs
- if available, before-after galleries of similar cases
- anything else you need to show the patient to help them understand the needed treatment.
Keep a folder aside on your computer that has pictures of things like broken teeth, perio condition, implants, etc.
If you’re presenting from the same computer every time, you can keep this folder on your computer.
But if you want flexibility from where you present treatment, then you can keep this folder on Google Drive / Drop box, make a shortcut on your Desktop – so you can pull it up anywhere through the office.
Let me tell you why all this is important.
Imagine you’ve just finished going over the clinical findings with the patient and now the patient goes to the front to meet the office manager.
As your manager is going over the treatment plan, don’t expect the patient to remember everything the doctor discussed in the operatory.
That’s why it’s important to show pictures of what you’re talking about while you’re discussing treatment.
But the manager doesn’t have access to the photos because they’re not attached to the chart yet. They’re still on the SD card on your camera.
Now the manager has to come back to the operatory, maybe let the assistant know to attach the intra-oral photos to the patient’s chart, so they have access at the front.
Transferring the photos from the SD card, then attaching to patients chart still takes a few minutes.
These steps matter.
This is all happening while patient is waiting at the front who was in the middle of discussing treatment.
It breaks the chain of thought, it’s a DISTRACTION.
Where to present treatment
When going over treatment, make sure to do it an area that is comfortable for the patient.
Patient should be seated.
Don’t make them stand at the front at check-out and then you see your treatment coordinator lean over the desk and going over the treatment plan with the patient while there are other patient in the waiting area.
It doesn’t have to be a closed room, but if your front area allows, don’t do it at the check-in area where other patients are seated and waiting.
Some patients will be uncomfortable with the entire situation.
Explaining Treatment
Before you start to explain treatment to the patient, make sure you’ve already spoken to the patient, gotten to know them a little bit.
Don’t expect patient to understand everything you say, so pause, and ask questions. While they’re answering, ACTIVELY listen and notice their body language – their apprehension, their anxiety, hesitation, etc.
Maybe you need to further address their objections to the treatment, and that objection maybe fear – either from their past experience, or maybe they heard something from a relative or a friend who had a bad experience with the same procedure..
Getting context is important
Here’s what I mean.
When you’re recommending a crown to a patient who has a large, leaky amalgam restoration – you’re going explain to the patient that it’s in their best interest to move forward asap before the tooth breaks and turns into a root canal.
Explaining why getting treatment done on time is important. Patients will often ask, can I do this in two months when i get back from vacation”? – Yo can’t make the decision for them, but just inform of the risk of waiting.
Yes, we want the patient to move forward with treatment as soon as possible, but what about the patient who has had a missing lower left first molar for last 18 years.
You’re not going to be able to say “if that molar isnt’ replaced soon”, X will happen.
From the patient’s perspective, if in eighteen years of that missing molar, if nothing has happened, and they’ve never bothered to move forward to replace that tooth – your recommendation of moving forward ASAP is just NOT going to do anything to drive the patient forward with getting the treatment done.
I remember in the beginning when I was a new grad, I’d sit down and see a missing molar and immediately jump to ask the patient “have you considered an implant?”.
And then go straight to “your back teeth are going to move and tilt towards the front and throw off your bite if you don’t replace it soon”
And I haven’t even talked much to the patient, have no idea of their previous dental history or experience, etc..
Patient’s response to this is: “that tooth’s been missing for 20 years, and i haven’t noticed any teeth moving”
And at that time, I’d just make a note in their chart and move forward with the exam.
But I could’ve avoided that situation if I hadn’t jumped into the treatment option – but instead asked questions in advance, so I’m better prepared to give options.
Ask for permission
If you’re seeing lots of abfractions, occlusal wear, gingival inflammation from calculus buildup on the lower due to anterior crowding –
You first state verbally what you’re seeing while you’re doing the examination.
Like the things I just mentioned, abfractions (say it in layman’s terms – breaks in enamel near the gum line), tooth wear, bleeding from tartar buildup due to overlapping teeth, etc.
Then, you ask for permission. “Would you be okay with me showing you some photographs of exactly what I’m seeing and reviewing how we can avoid further damage to the teeth and how we can make it easy for you to keep things clean?”
Patients 99% of the time always appreciate this, because you’re spending more time and not being pushy like their previous dentist – and they’ll say yes.
Once you take the photographs, now it gives you an opportunity to discuss treatment options such as mouthguard and orthodontic treatment to correct the crowding.
Using Dental analogies
Once you’ve gotten to know the patient a little bit, you can ask the patient what they do for a living.
Many times, the patients usually just tell you because they’re sharing their story of what’s been going on in their life or earlier in their day or the week, etc.
If you’re actively listening, keep this information in mind and if you can somehow relate the treatment they need to something in their line of work – they’re better able to understand why they need the procedure and risks of not moving forward.
If they understand what’s being done, they’re more likely to move forward..
Some examples:
When I’m explaining why the patient needs SRP, I don’t say they have periodontal disease, or gum disease. I say gum infection.
I mention words that THEY themselves use to describe their gums.
You often hear patients say, “my gums bleed while I’m brushing sometimes”, or “it hurts in some areas when I try to floss”, etc..
You want to use trigger words like infection, pus, blood, pain, etc.
When explaining why they need bone grafting at the time of extraction – don’t say words like “preserve bone”, or “socket preservation” – I usually let them know that by placing bone into the space where the tooth was, you’re preparing it for the future implant tooth.
To make sure there’s enough scaffolding and support around the implant, you have to place the graft material, otherwise, there won’t be enough bone to support the implant and it can fail.
Instead of going over all the different analogies – I’ve put together a separate PDF which you can keep handy. You can download it by clicking on the link below this video!
Follow a simple framework for consistency:
An ideal treatment plan is always a combination of your findings during your clinical examination, and patient’s perceived need or chief complaint.
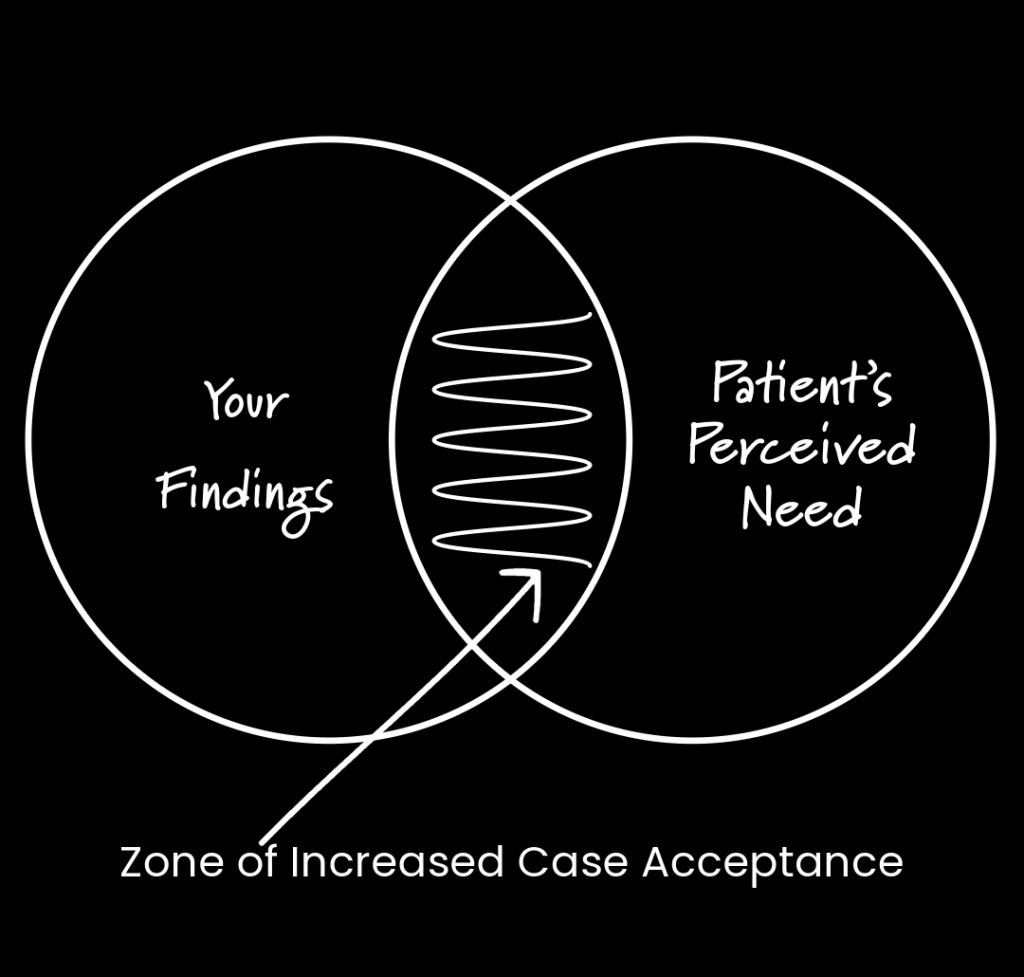
By doing this consistently, you’re going to become better and better as you practice and improve on this – you’ll get greater acceptance rate.
Here’s what I’m talking about:
To address the [state their complaint] [from/due to], [ state cause here], [state tx option] will be an ideal option to [state what tx achieves], so your [state perceived need].
You don’t have to use this sentence in the exact format, but however, you’re going to put it to the patient – it needs to include the following points:
- Their chief complain or their perceived need
- What caused the issue
- Treatment option
- What the treatment option achieves
- what does it look like / feel like for the patient??
Making sure the team is trained on explaining treatment to patients
I can say this with 100% confidence that in most offices, there will always be team members who are not able to explain the importance of a treatment procedure to a patient.
This is true whether they’re part of the clinical team, or the front desk team.
This happens all the time especially when diagnosing a mild to moderate perio patient – who really needs to come in for scaling and root planing, but instead are only scheduled for their prophy every 6 months.
So when the team members aren’t trained or are unaware themselves of the importance of the treatment – they’re going to opt for the path of least resistance out of fear of upsetting or losing the patient.
The only way to fix this is to role play with the team members.
Train them not only how to explain the treatment in layman’s terms, but to also address patients’ objects to moving forward with treatment.
Asking questions
While you’re presenting treatment, or even at the end of the treatment – you should be asking questions that require the patient to think about the answer.
Don’t ask questions that can be answered with a simple yes or no.
Avoid questions like “Do you understand”? or “Any questions” – patients will just say “yes”, when they really do not.
Instead, what I ask the patient is this: “”knowing all the risk of not moving forward with what we’ve recommended, what’s stopping you from getting this done?”
Summary of Best Practices
Remember the goal is to make sure patient has an appointment on schedule.
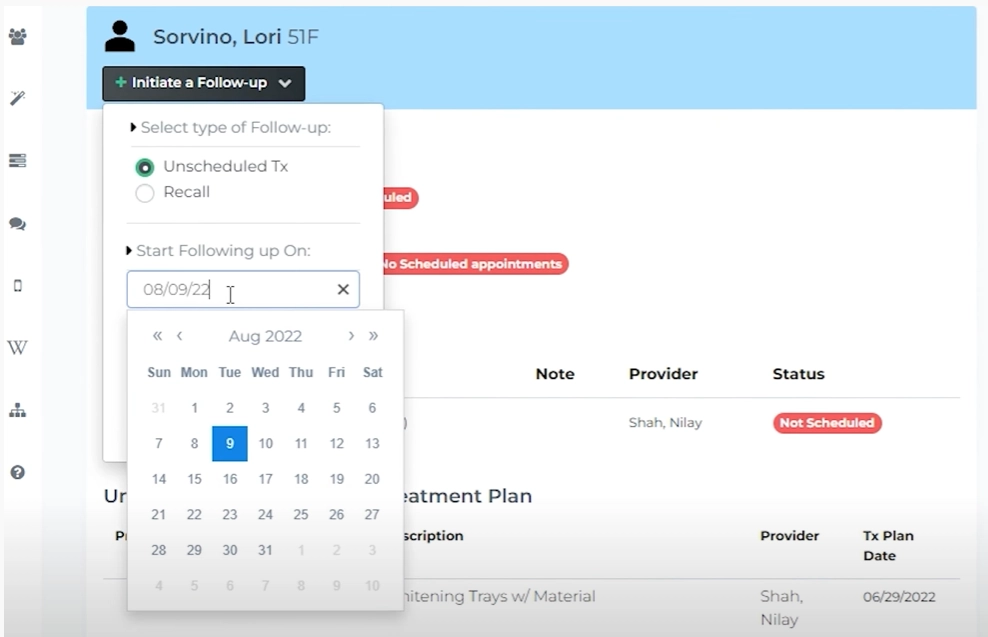
If they don’t schedule, you need to set a follow-up either manually.
Or if you’re using Teamio, set up a follow-up date from the patient profile or from the Unscheduled treatment page via search.
Don’t take things personally. You have to understand that just because a patient doesn’t move forward with treatment now, doesn’t mean they’ll never move forward.
I’ve had patients that have waited two, three, and sometimes more prior to moving forward with major treatment.
But what’s important is that you recall, re-iterate, re-emphasize at their hygiene visits, on the importance of the unscheduled treatment.
As mentioned earlier, ideal treatment plan is always a combination of your findings during your clinical examination and patient’s perceived need or chief complaint – you’re going to get higher case acceptance with patients this way.
Other helpful resources related to Treatment Planning
If you haven’t read the post on Financial Arrangement and Treatment Planning, I recommend going through it because I talk about how I approach patients who may have larger treatment needs.
From the post, you’ll also be able to download treatment plan templates that I use on a daily basis in my practice.